20 min read
No one knows, and no one will ever know, exactly how many medical doctors fled Syria as the protests of 2011 morphed into a civil war that continues to this day, pushing the country’s health system into collapse. As Syrian physicians sought refuge across the world in 2011-22, no country kept reliable records of their presence
Arab Reporters for Investigative Journalism (ARIJ) can prove that the true extent of the exodus is larger than what the Syrian government and multinational institutions have officially reported. So are its implications for the rest of the world, as highly skilled refugees from Afghanistan, Ukraine and elsewhere choose the path of exile.
Before going further, it’s worth recalling that in 2010, Syria could be considered a model of health care development.
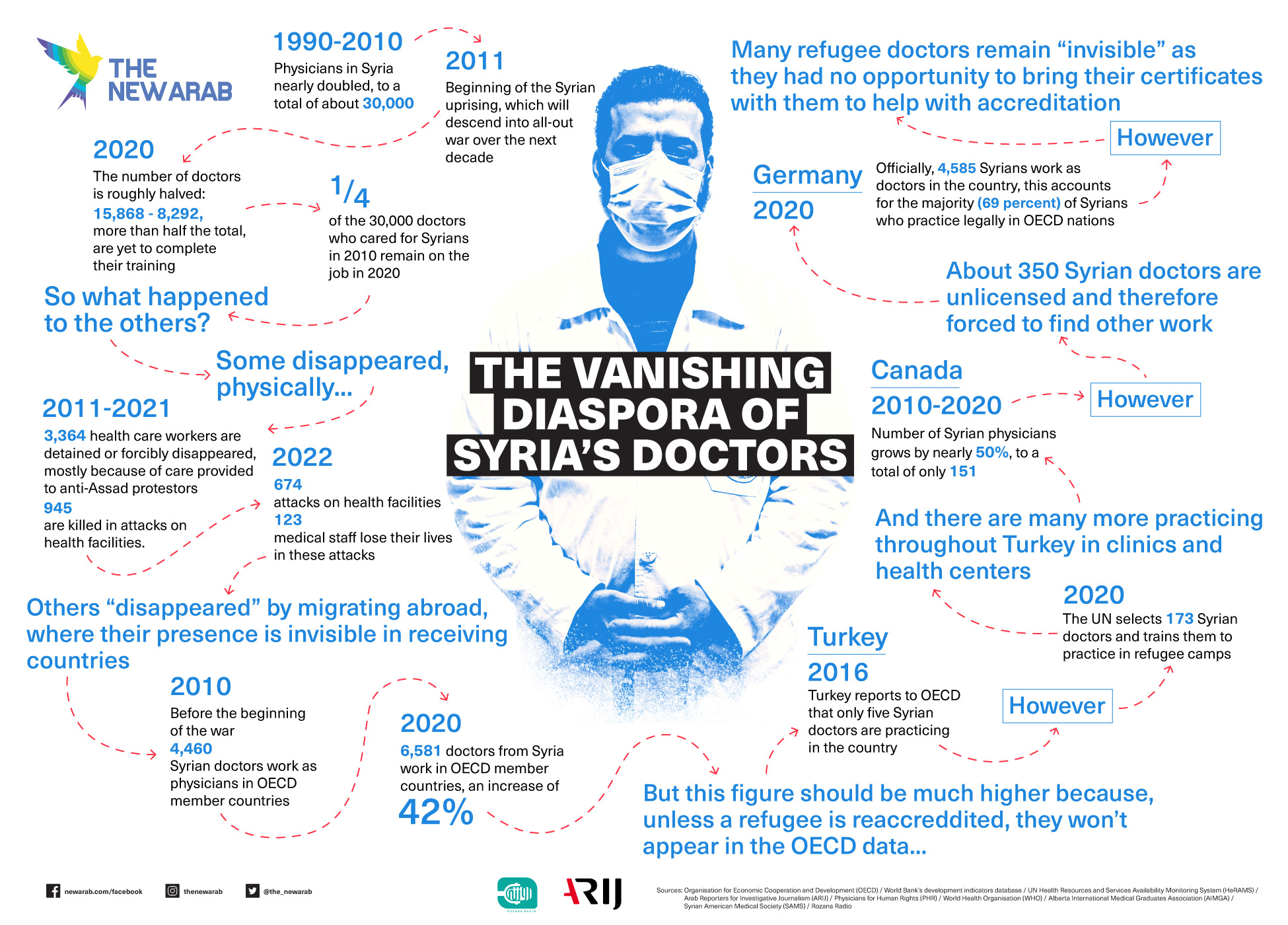
A flourishing pharmaceuticals industry supplied 90 percent of the country’s needs for medications. From 1990 until 2010, the number of physicians serving the population nearly doubled, according to the World Bank’s development indicators database, to a total of about 30,000. They were an intellectual, social and political elite. To join the faculty of a medical school, “loyalty to the Baath party is one of the conditions,” said Dr. Hussam Al-Nahhas, Middle East and North Africa (MENA) Researcher at Physicians for Human Rights (PHR). “A faculty member cannot be the head of a department or even the dean without being closely affiliated to the party.”
The system did also have gaps and shortcomings. Students were trained to treat diseases, rather than to prevent them – a problem for a country where chronic diseases like diabetes account for most deaths. To supplement their public sector pay, physicians started clinics that served wealthier citizens as well as medical tourists from the Middle East to Moscow; low-cost plastic surgery became a Syrian specialty, especially in Damascus.
"Documenting qualifications can be extremely difficult for physicians in flight: Refugees arriving from Syria often had no opportunity to bring certificates with them.”
Meanwhile, a disaster was underway.
Uprising and war
A month after protests against repression and corruption within the government of President Bashar al-Assad erupted in March 2011, demands for reform turned into calls for revolution. In response, Assad unleashed his army against his fellow citizens in about 20 cities.
Physicians were quickly faced with a dreadful dilemma. Medical ethics as well as international treaties that Syria had signed required that they care for protestors who had been harmed by the army and security forces. But the government viewed any doctor who helped protestors as an enemy of the state. A doctor quoted by Physicians for Human Rights, was told by his Syrian interrogator, “You are far more dangerous than terrorists. We kill them, you bring them back.”
In the first year of the uprising, Assad’s services detained 44 Syrian physicians for providing medical help to protestors, according to PHR. Four of them died in prison, and 22 disappeared in the security system and were never found again. There would soon be hundreds more.
At the time Dr. Al-Nahhas was among a group of young physicians in Aleppo, who called themselves Noor Alhayat, “the light of life”. They sought to provide care as the government hunted patients and physicians. Al-Nahhas told us: “The government increased the security presence in these hospitals to capture anyone who got injured during demonstrations.” It became unsafe for protestors or wounded bystanders “to go to any private or to any public hospital,” he said.
To buy time to “stabilise people’s injuries” before security agents appeared, said Al-Nahhas, it was typically necessary to create a “fiction” about how the wound occurred, “to bring the story away from the fact that this person was participating in a demonstration.” In one case, a boy whose leg had been mangled by a grenade was told to tell the agent who came to interview him in the hospital that “a huge iron door fell over his body and damaged his leg.”
Such tactics didn’t work for long. In June 2012, “three of our volunteers were captured by the state intelligence [forces],” said Al-Nahhas. “And after a few weeks of being detained, they were sent back to their families, burned. They were tortured, killed under torture, with bullets in their heads.” That July, Al-Nahhas was arrested in turn. He was released after 17 days through his family’s connections, he said. In the meantime he was tortured. Soon after, he fled Syria for the US.
From 2012 through 2015, another 550 medical personnel were likewise arrested, according to PHR. The number kept rising. By 2021, the organisation calculated that 3,364 health care workers were “detained or forcibly disappeared.” An additional 945 were killed in attacks on health facilities.
Beginning in 2015, the Syrian state and its Russian allies unleashed a campaign of targeted destruction against health facilities in rebel-held areas. The Syrian American Medical Society (SAMS) documented 674 attacks on health facilities through 2022, of which 91 percent could be reliably credited to Russian or Syrian forces. SAMS reported: “480 individuals – 123 medical staff and 357 patients – have sadly lost their lives in the documented attacks. 56 of those were children. In addition to death, 1268 individuals – 318 medical staff and 950 patients – have been injured. 137 of those were children.”

State terror was the main threat to physicians and their patients in Syria, but it was not the only terror they faced. Chaos enveloped the country in 2014-15, as the Islamic State and other militias sought to wrench territory from the government. Kidnapping for profit was among the militias’ fundraising methods.
Christian Vitale, a general practitioner with decades of experience in Syria, faced that threat. He is now a Canadian citizen, working as a case manager for health in the Center for Newcomers in Calgary, helping refugees “to find health resources,” he told us. In 2015, opposition groups in his native Latakia, a province now entirely under government control, “tried to kidnap my son,” he said. “They targeted sons of doctors, engineers, kind of known people in the city, who they suppose have money.” He said he personally knew of two cases where “they kidnapped the kids and killed them, took the money and killed them… and sent bodies, dead bodies to their families.” It was the reason he left Syria with his family in 2015.
Economic collapse
A third threat to physicians emerged with the collapse of the Syrian economy, as international sanctions and inflation hammered the national currency. We interviewed five physicians within Syria, aged 24 to 39, here identified by their first names for security reasons. They told us that the conditions of their lives and work had become very difficult.
First, they had been reduced to poverty. Sanctions against Assad’s government, among other factors, have destroyed the value of the Syrian pound, currently trading at 13,000 to the dollar; ten years ago, 104 pounds bought a dollar. One of the five doctors, Siraj, said that his salary did not cover his basic needs, including transportation from his home to the hospital. Rents, he said, had become “unaffordable,” even for doctors.
He looked at Syrians abroad with envy: “All these doctors outside the country, they will be productive people. In Syria, doctors will be completely consumed and completely dependent on their families, unable [...] to advance their lives and futures, unable to establish a family.”
Another common complaint is the deterioration of the hospitals and clinics where doctors operate. There are “no medicines, no hygiene,” said Jawal. In his hospital, he added, “the elevators are out of order, and the maintenance workshops are not working.” Hussein told a similar story: “There is a shortage of equipment and medicines due to the sanctions, and sometimes even the maintenance equipment seems to be difficult to maintain.
"Refugee physicians are badly needed in the West at a time when budget cutbacks lead to catastrophes like the COVID health care breakdown.
Exodus
Meanwhile, Syrian physicians fled by the thousands – to Jordan, Lebanon, Turkey, the Gulf States, Europe, North America, the Caucasus, and to countries all over the world.
How many, exactly? No one can say with certainty. There is no international system that collects data from refugees about their professions while they are in camps or awaiting decisions from asylum authorities. The bottom line is nonetheless clear: thousands of Syrian physicians vanished into interminable waits for accreditation abroad, other professions or clandestine practice, and have never been accounted for. It’s as if they climbed over a wall to leave Syria and slammed into another one.
One way to estimate their numbers lies with the United Nations’ Health Resources and Services Availability Monitoring System (HeRAMS) data, which has been compiled since 2018 in Syria. The data is collected by “a team of national health staff from all governorates”, to make up for “the shortage of timely and relevant information,” according to the UN. That means it isn’t perfectly accurate. It is nonetheless very revealing.
2020 was the only year for which the UN collected data covering a wide scope of health facilities in wartime Syria – public hospitals and “health centres”, private hospitals in the Al-Hasakeh province beside the Turkish border, NGOs, the Red Crescent, and the UN’s own medical outposts. That year the total number of general practitioners, surgeons, emergency physicians and various other specialties came to 15,868 people. That was about half the number of physicians working in Syria as of 2010.
Equally striking, among the doctors counted by the UN, no less than 8292, more than half the total, were residents – physicians completing their medical training by working with patients. This can be read as evidence that the Syrian state made an accelerated effort to replenish the ranks of its shattered medical corps.
It also suggests that only one-fourth of the 30,000 doctors who cared for Syrians in 2010, according to the World Bank’s Development Indicators database, remained on the job in 2020. Where did the other tens of thousands go?
The Organisation for Economic Cooperation and Development (OECD) tracks physicians who immigrate in order to practise in its member countries. The OECD extracted data for us concerning Syrian physicians from 20 nations, covering the years 2006-2020. That data leaves out countries like Malaysia or the United Arab Emirates, where Syrian practitioners are highly visible. But for developed nations, it’s the best data we have.
According to the OECD, in 2010, before the war began, a total of 4640 doctors from Syria were working as physicians in member countries. By 2020, the last year in the database, the number was 6581, an increase of 42 percent. It’s a smaller number than we’d expect, given the tens of thousands who fled Syria.
However, the data is riddled with glaring holes.
The biggest is that a doctor doesn’t stop being a trained physician when they become a refugee; however, unless they are re-accredited to practise in the country of arrival, these professionals never appear in the OECD data.
Turkey
Turkey offers a flagrant example. It reported to the OECD that through 2016, a total of five Syrian physicians were practising in the country; no new data have been reported since then. When told these numbers, Sahar Nohni, project manager at Canada’s National Newcomer Navigation Network (N4), a non-profit organisation, reacted: “I personally know 20.”
In 2020 alone, the United Nations selected 173 Syrian physicians in refugee camps in Turkey and gave them training that allowed them to practise in the camps. The initiative required a special arrangement with the national medical society, which “did not support this program”, said Sarada Das, secretary general of the Standing Committee of European Doctors (CPME), which includes Turkey. Those 173 physicians do not appear in Turkey’s reports to the OECD.
In parallel, clinics, health centres and laboratories operated by Syrian doctors and Syrian health care professionals have mushroomed in Turkey and especially in Istanbul. They work under licence and nominal supervision of Turkish doctors, without being accredited as doctors themselves. Most of the physicians live in Turkey under a refugee status or short term (renewable) residency permits that do not mention their professions, while most of the clinics are outpatient, dental and plastic/reconstructive surgery clinics.
This comes at a time when Turkey is promoting itself as a new hub for medical tourism and is aiming at a $20 billion in revenues from this sector for 2023. In 2022, 1,700 foreign patients visited the country, spending $12 billion according to MedicalPark Hospitals, a national chain of high-end hospitals and medical facilities.
“Canada accepted them as immigrants based on ‘Oh, you're a nurse or a physician, you'd be a great asset to Canada, welcome to being a Canadian citizen.’ And then they're kind of left on their own.”
Lebanon
An underground Syrian medical sector also appeared in Lebanon. In 2018 the Syria Public Health Network (SPHN), a coalition of researchers based in the UK, reported “the emerging phenomenon of qualified Syrians carrying out informal healthcare work to meet local needs”.
At the time 1 million Syrian refugees were registered in Lebanon, and another half-million were known to be there, according to the United Nations High Commission for Refugees. Their health needs were acute, particularly for chronic diseases related to stress – hypertension, diabetes, cardiovascular problems.
However, “Syrian refugees often find it very difficult to afford the care they need in Lebanon’s highly privatised healthcare system”, noted the SPHN authors. Refugee health care workers filled the gap through the black economy. The SPHN interviewed 40 of them. They spoke of the difficulty of obtaining accreditation or work permits, “persistent fear and distress (including threat of deportation), ethical challenges, discrimination and inability to make a living”.
"Neither could afford to obtain re-accreditation in Canada – a process that amounts to a second full-time round of medical education – and both took other employment."
Canada
Canada, a main destination for Syrian exiles, offers insight into the gap between official numbers and reality. The country is facing an acute shortage of the family practitioners that the Syrian medical system excelled in training. According to the OECD, from 2010 until 2020 the number of Syrian-born physicians in the country grew by nearly 50 percent, to a total of only 151.
Multiple sources confirmed to us that this figure is a steep understatement, and that Canada has never integrated hundreds of Syrian physicians into its corps of practitioners.
Christian Vitale is one of the doctors who remains unaccounted for by the OECD, and he says he knows plenty of others. He was a family doctor in Syria; his wife was trained and practised there as a gynaecologist. Neither could afford to obtain re-accreditation in Canada – a process that amounts to a second full-time round of medical education – and both took other employment.
He explained: “I came with some English….I had to learn fast to get a job and to support my family. [...] We spent a lot during the first year, second year. And I had two boys at the university. And my wife was studying, she did a master's in health management. I didn't have the privilege to stay at home and study for two or three years to get my credentials. The system here is even if you get your credentials, you pass all the exams and the English test, after that you have to do two years of residency to become a family doctor.”
Vitale said he personally knows ten other Syrian doctors in Calgary who faced the same situation. He added that “there are a lot, hundreds maybe, from other cities.” Vitale himself belongs to a WhatsApp group of Syrian physicians with 150 members back home and abroad.
Other sources agree with him. Deidre Lake, director of the Alberta International Medical Graduates Association (AIMGA), an advocacy and support group with 1,600 active foreign-trained physician members, said that, based on annual surveys of AIMGA membership, 70 percent of Syrian exile doctors never obtained their credentials in Canada. Using the OECD count of 151 Syrian doctors who are licensed in Canada as a benchmark, that means about 350 were forced to find other work.

Similar data comes from Canada’s National Newcomer Navigation Network (N4), which conducts courses for foreign-trained professionals “looking to be optimally employed and thrive in the Canadian Healthcare system”. In 2022 N4 was overwhelmed by demand from potential participants. “We got more than 300 applicants, but we are going to be accepting only 60. So what can you do?” said Christine Kouri, N4’s director.
She sees a tragic irony in the situation. “Canada accepted them as immigrants based on ‘Oh, you're a nurse or a physician, you'd be a great asset to Canada, welcome to being a Canadian citizen.’ And then they're kind of left on their own.” The result, she said, is that “only about 40% are successful to work within their professions."
"Some of the refugee physicians are selling their cuisine in the street markets. A tragedy. A real system [to accredit the exiles] isn’t in place.”
Dr. Annalee Coakley is medical director for AIMGA and a determined advocate for refugee patients and practitioners. She makes an argument that is shared by the Syrian Public Health Network in the UK: Western health systems have made it practically impossible to integrate every refugee physician who might contribute to their receiving country’s well-being, and those physicians are badly needed at a time when budget cutbacks lead to catastrophes like the COVID health care breakdown.
Coakley saw that firsthand when COVID raced through Canada. “In Calgary our internationally trained physicians were key to addressing the outbreak at the Cargill [High River] meatpacking plant, for example,” she said. That was the single biggest outbreak of the pandemic in North America. Those doctors, who were not licensed to practise or treat illness in Canada, nonetheless provided crucial services like a “first look”, when the patient’s physical condition – the colour of the skin and eyes, the warmth of the skin, their energy and strength – was assessed.
She said hopefully, “the government is looking at ‘how do we scale this up?’ And also, what are the barriers [exile physicians] face to credentialing? You know, there's a deficit of care across Canada, so how do we help overcome some of these barriers that they face?” Then she said: “Because in Canada, there's a ton of barriers that they face, that make absolutely no sense.”
The main one is time, and in Calgary, the time is getting longer. There, the Alberta Medical Association has just introduced a mandatory “externship” of three months under the supervision of a Canadian physician. The supervisor’s assessment alone determines if the candidate will be accredited. A two-year residency is required beforehand, and there are not enough residencies to absorb all candidates. Canadian-educated candidates are preferred.
The effect is that in Canada, the gateway to integrate foreign-trained physicians is narrowing. “You know, we're fighting,” said Coakley. “We're fighting. You know,” she said, and struggled to find the right term before concluding: “The difficulty”.
"Thousands of Syrian physicians vanished into interminable waits for accreditation abroad, other professions or clandestine practice, and have never been counted. It’s as if they climbed over a wall to leave Syria and slammed into another one."
European Union
Similar factors are at work even in Germany, which alone accounted for 69 percent of all the Syrian-born physicians who practised legally in OECD countries as of 2020 – a total of 4585. Germany is “the way for everyone,” said Ahmad, a surgeon in Damascus. Farah, a recent medical school graduate in Damascus, told us: “I have many colleagues who are thinking of travelling, and the destination is mostly Germany. You will get tired if you want to find someone who says otherwise.” Ahmad marvelled that his exiled peers in Germany “were able to adjust and started specialising within two years”. But there is reason to doubt this optimistic image.
In a 2020 study, the University of Regensburg's Institute of Medical Sociology starkly described the explicit and implicit barriers to the integration of Syrian doctors in the German health system:
“All interviewees described the licensure process as a complex, lengthy, ever-changing and non-transparent procedure, which is perceived as a partly unfair, sometimes arbitrary bureaucracy. They often feel at [the] mercy of Government employees and report experiences with reviewers who ask for absurd and impossible accomplishments, refuse to give information, and act at random. […] The interviewees describe themselves as depressed, irritated and/or in despair.”
The Standing Committee of European Doctors (CPME), who represent medical associations across the EU, “oppose fast tracks [for accreditation] that reduce the level of scrutiny“ of candidates, said Secretary General Sarada Das. “From our members’ point of view this creates second-class healthcare. Every patient should be able to rely on the fact that their HCP [health care provider] has undergone necessary training.”
She acknowledged that documenting qualifications can be extremely difficult for physicians in-flight: “Refugees arriving from Syria often had no opportunity to bring certificates with them."

Françoise Henry, director of the section for training and competencies of the Council of the French Order of Physicians, said that the obstacle for Syrian exiles was the absence of “equivalent diplomas” between Syrian and French medical schools. In France, she said wearily, “we only recognise diplomas.” Henry reportedly tried, and failed, to persuade the Ministry of Health to recognise that the Syrians were “perfectly competent, at a very good level, after studies similar to [those in] France”. She was particularly impressed by their clinical skills: “They had that experience.” Her appeal fell on deaf ears and had no impact on French policy.
"No international system collects data from refugees about their professions while they are in camps or awaiting decisions from asylum authorities."
Cultural and language barriers
Syrian physicians also ran into cultural barriers. In the German study, “All three interviewed female doctors reported that their wearing a Hijab led to episodes of discrimination in their job search.”
In Canada, Christine Kouri of N4, who created a partnership agreement to facilitate residencies for foreign-trained doctors, said that “one issue was getting calls at least once a week from a woman who was personally offended. We had some Saudi residents come for orthopaedics, and the moms said, ‘That resident would not shake my hand. They're sexist, blah, blah, blah,’ I'd get an earful. So we had to do some interventions for [the residents] to explain, ‘I am not going to shake your hand, because in my culture, that's disrespectful, and I don't want to disrespect you.’ Then [the women would say], ‘Oh, great, that's not a problem.’
“But in the end, we actually ended that partnership,” said Kouri. “It just couldn't be overcome. I don't think [the partners] put the resources into the training of these poor fellows who were well-meaning, great clinicians.”
The ultimate barrier for exile physicians is language – professional, bureaucratic and personal. Typically, a language test is the final step before accreditation. Standards vary from country to country: “This is regulated at the national level,” noted Sarada Das, of the Standing Committee of European Doctors. In any country, language requirements for certifying professionals go far beyond typical conversational skills. Different countries use different terms for the same medical procedures. There are documents and online forms to complete for patients. Most importantly, the patients express their concerns in their national languages. “It’s important to communicate with families and other professionals,” said Das. “It’s a patient safety issue. Since the pandemic we’ve seen that this also applies to online communication, for tele-medicine. There is a relatively high standard expected.”
Those expectations are known to medical students in Syria today. Vitale, the exile physician in Canada, said: “The majority of them [are] studying English, or German, or other languages, because [they have] the intention to leave the country after graduation. Because there is no hope there."
"A doctor quoted by Physicians for Human Rights, was told by his Syrian interrogator, 'You are far more dangerous than terrorists. We kill them, you bring them back.'"
Foreign doctors: A solution for battered health systems?
There is hope for a change in the situation of Syrian exile health workers The combined crises of health funding cutbacks, COVID and Ukraine have compelled national medical authorities to rethink the practice of excluding foreign professionals. “Mostly the dominant problems are that shortages and lack of capacities persist, and the burnout rates increased [during the pandemic],” said Das, the CPME secretary general.
Economic factors support this trend. The Syria Public Health Network (SPHN), founded in the UK in 2015, has long argued that exile physicians represent a relatively low-cost solution to shortages of doctors. “It will cost at least half a million pounds to train a UK medical student from undergraduate through to a consultant,” said Aula Abbara, a physician and steering committee member at the SPHN. “But if you take in [...] a Syrian doctor or Ukrainian doctor who has gone through medical school, it's less than half the cost.”
This point was echoed by Das. It “is also coming up in the Ukrainian situation, especially for nurses,” she said. “Many have arrived in European countries with more comparable qualifications, and they have been given access to the labour markets right away. That was denied to Syrian refugees. They were excluded from the labour market for a long time.”
“Evidently, France needs these physicians,” said Françoise Henry of the French Order of Physicians. The supply of doctors is inadequate to serve public needs, she said: “All of Europe is in a situation of crisis. That’s why we tried to help the exiles.” But for the moment, little has changed, she said: “Some of them are selling their cuisine in the street markets. A tragedy. A real system [to accredit the exiles] isn’t in place.”
While awaiting these changes, this remains the story of untold waste – of ideals, of talent, of lost opportunities, and of skills that could save lives. Syria made it impossible for doctors to use those assets at home. Ultimately, nothing makes it impossible to use them abroad.
Disclaimer: This investigation is co-published with Arab Reporters for Investigative Journalism (ARIJ) and Radio Rozana, but The New Arab Investigative Unit was not involved in the development of this project. All related questions should be therefore addressed to ARIJ (Editor@arij.net). Click here to read the Arabic version.

![President Pezeshkian has denounced Israel's attacks on Lebanon [Getty]](/sites/default/files/styles/image_684x385/public/2173482924.jpeg?h=a5f2f23a&itok=q3evVtko)



 Follow the Middle East's top stories in English at The New Arab on Google News
Follow the Middle East's top stories in English at The New Arab on Google News